





Sleep apnea is a condition where breathing repeatedly stops and starts while you sleep.
Each pause can last a few seconds to over a minute, and it can happen dozens of times per hour without you knowing.
The pauses occur because something is blocking the airway or the brain is not sending the right signals to the muscles that control breathing.
When oxygen drops, the brain triggers a brief wake-up to restart normal breathing, often so brief you have no memory of it.
The main types include obstructive, central, and complex sleep apnea, as well as sleep-related hypoventilation.
Identifying which type you have is the first step toward effective treatment, since each one responds differently to therapy.
Medical disclaimer: This article is for informational purposes only and does not replace medical advice. Always consult a qualified healthcare provider for diagnosis or treatment.
What Are the Severity Levels of Sleep Apnea?
Sleep apnea severity is measured by the apnea-hypopnea index, which tracks how many times breathing is interrupted per hour of sleep.
| Severity Level | AHI Score | Common Symptoms |
|---|---|---|
| Mild | 5 to 14 | Light snoring, occasional fatigue, minor concentration issues |
| Moderate | 15 to 29 | Loud snoring, morning headaches, significant daytime sleepiness |
| Severe | 30 or above | Extreme fatigue, memory issues, elevated blood pressure, mood changes |
Your AHI score determines not just treatment intensity but also your long-term health risk.
What are the 4 types of sleep apnea?
Not all sleep apnea works the same way.
The condition is generally classified into four main categories based on how breathing is disrupted during sleep.
1. Obstructive Sleep Apnea (OSA)
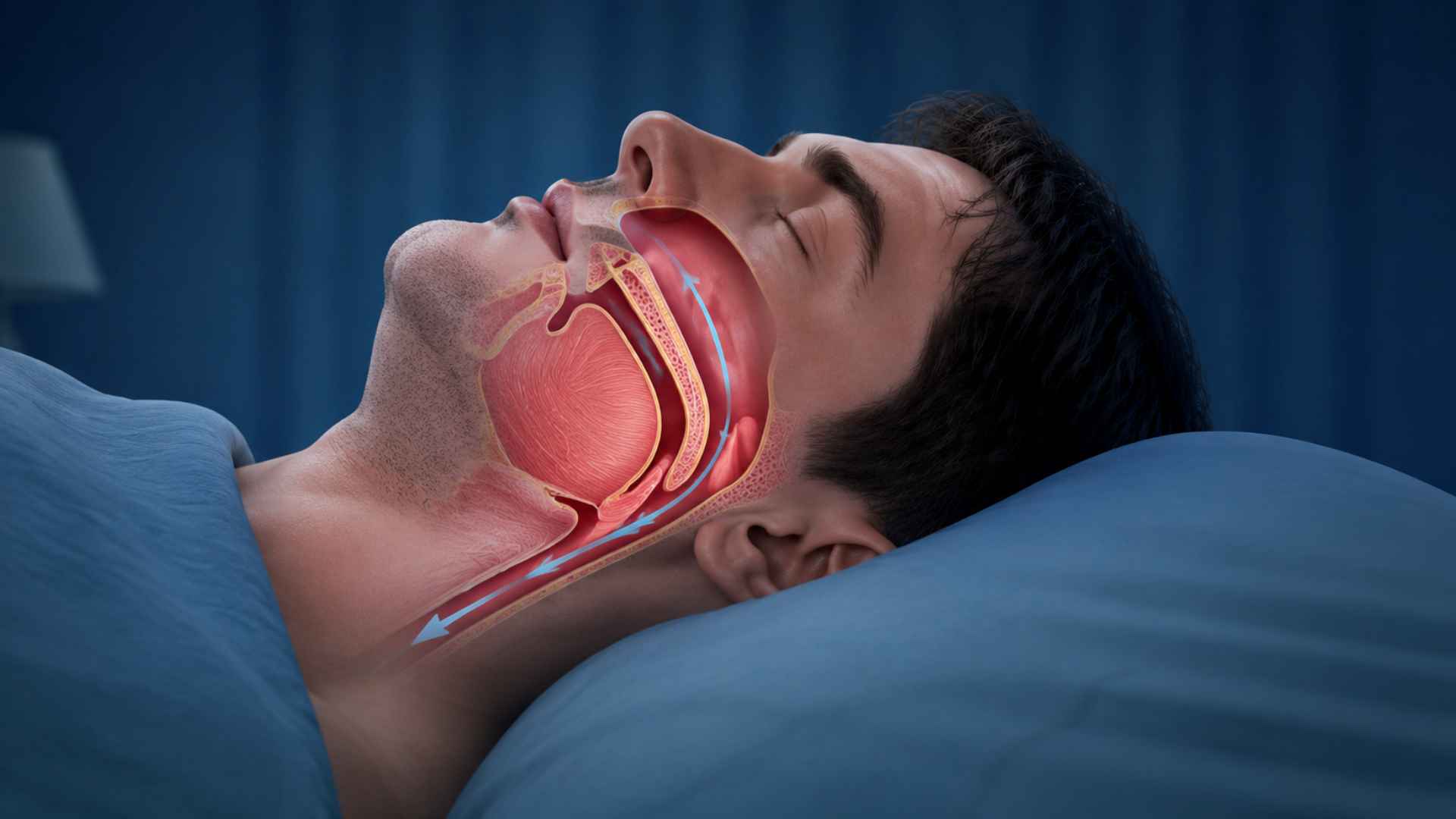
Obstructive sleep apnea is the most common type.
In people with OSA, the muscles in the back of the throat relax during sleep, reducing space for air to pass through, a process widely described in clinical sleep medicine literature.
In many cases, these airway blockages are also linked with unusual nighttime experiences described in sleep apnea dreams.
The brain eventually detects the drop in oxygen and sends a signal to wake the body just enough to reopen the airway.
This cycle can repeat dozens of times per hour, and most people have no memory of it happening.
2. Central Sleep Apnea (CSA)
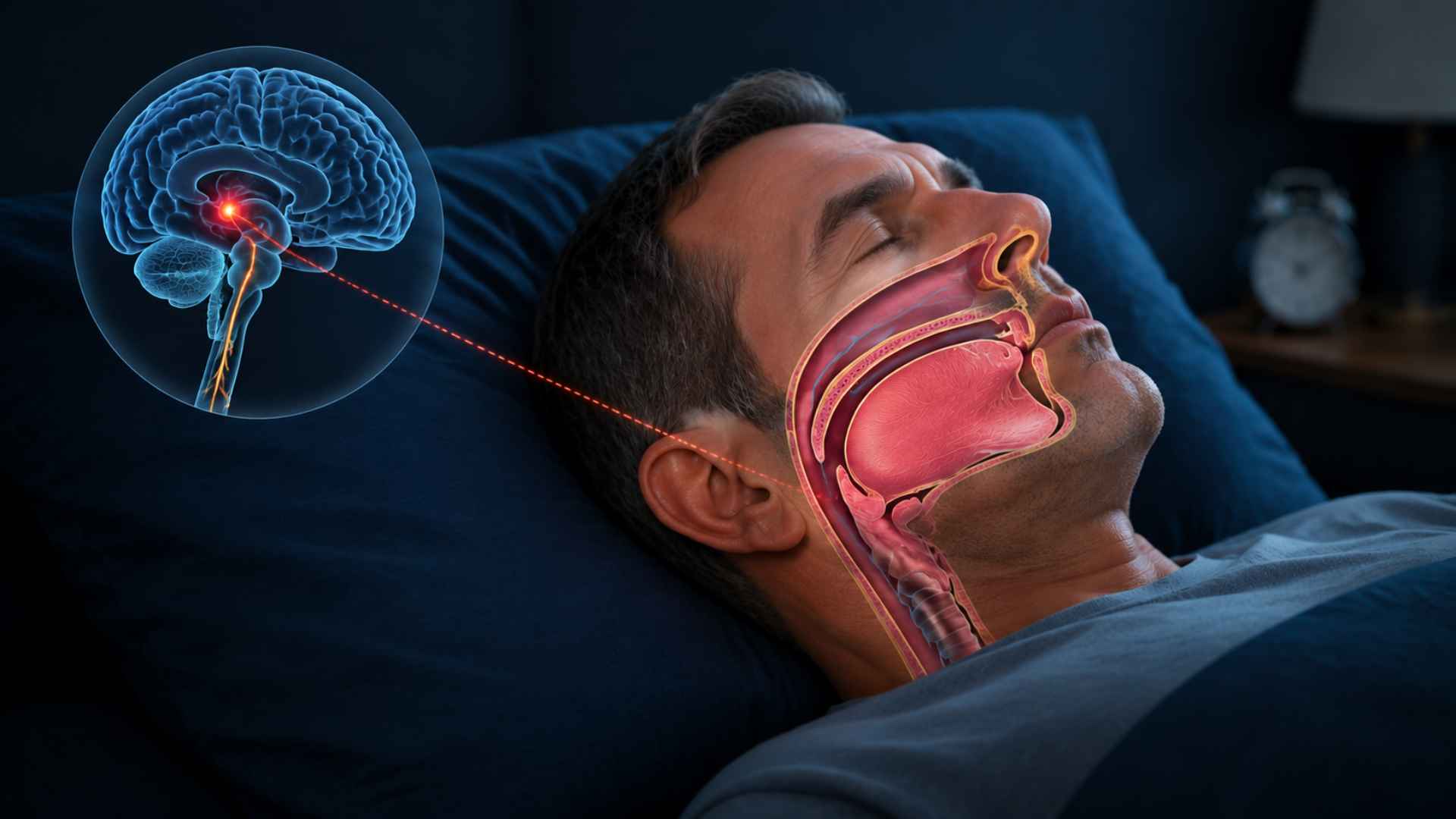
Central sleep apnea is less common and works differently from OSA.
The airway itself is not blocked, but the brain fails to send the correct signals to the muscles that control breathing, so breathing simply does not happen for a period.
It is often linked to underlying conditions such as heart failure, stroke, Parkinson’s disease, severe kidney failure, or the use of certain medications.
Because central sleep apnea is often linked to underlying neurological or cardiac conditions, it may in some cases contribute to disability evaluations depending on severity and associated impairments.
As the cause is neurological rather than physical, treatment approaches differ significantly from those used for OSA.
3. Complex (Mixed) Sleep Apnea

Complex sleep apnea, sometimes called treatment-emergent central sleep apnea, involves both obstructive and central patterns.
It is typically identified when a person being treated for OSA continues to show central apnea events even after the airway obstruction has been addressed.
Managing this type requires a more layered approach, as both the physical blockage and the signaling disruption must be accounted for in the treatment plan.
4. Sleep-Related Hypoventilation (Related Disorder)

Sleep-related hypoventilation is a broader category where breathing does not stop completely but becomes too shallow or too slow to move enough air through the lungs.
This leads to a gradual buildup of carbon dioxide in the blood rather than the sharp drops in oxygen seen in other types.
It is most commonly associated with obesity, chronic lung conditions, or neuromuscular disorders that affect the muscles involved in breathing.
Clinicians use this classification when breathing patterns involve sustained hypoventilation that is not fully explained by obstructive or central sleep apnea criteria, often seen in conditions like obesity hypoventilation syndrome.
The likelihood of each type can sometimes be influenced byfamily history of sleep apnea, especially in obstructive cases.
Common Signs of Sleep Apnea
Sleep apnea does not always wake you up fully, but your body leaves clear clues.
Clinical descriptions of what sleep apnea is and how symptoms appear during sleep are also outlined in major health research summaries.
These are the most common signs to watch for:
- Loud, irregular snoring that stops and starts through the night, often followed by a sudden snort or gasp as breathing resumes.
- Gasping or choking during sleep when oxygen drops low enough to trigger a partial wake-up response.
- Waking up with a dry mouth or sore throat from a night of mouth breathing when the airway is partially blocked.
- Morning headaches occur when low blood oxygen and rising carbon dioxide levels cause blood vessels in the brain to dilate, building pressure that lingers into the morning
- Daytime fatigue despite a full night of sleep because sleep apnea deprives you of access to the deeper, restorative stages of sleep.
- Difficulty concentrating or memory lapses from a brain that never got the overnight recovery it needed.
- Mood changes, such as irritability or low motivation, that build over time with chronic poor sleep.
If any of these signs feel familiar, talking to a doctor is the right next step. A proper diagnosis can make a significant difference in how well you sleep and how you feel during the day.
How Sleep Apnea is Diagnosed
Diagnosing sleep apnea starts with a sleep study. There are two main options depending on your situation:
1. Polysomnography (in-Lab Sleep Study)
Conducted overnight at a sleep clinic, this is the most thorough option available.
- Monitors brain activity, oxygen levels, heart rate, breathing, and body movement simultaneously.
- Recommended for complex or unclear cases that need a detailed evaluation.
2. Home Sleep Apnea Test
A simpler alternative that lets you complete the test from the comfort of your own bed.
- Tracks breathing, oxygen levels, and airflow using a portable monitoring device.
- Best suited for straightforward OSA cases and is easier to access for most people.
Both tests measure how often breathing is interrupted per hour, recorded as the apnea-hypopnea index.
An AHI below 5 is considered normal, 5 to 14 indicates mild sleep apnea, 15 to 29 indicates moderate, and 30 or more is classified as severe
A doctor uses that number, along with your symptom history, to confirm a diagnosis and identify the type of condition.
Treatment Options for Sleep Apnea
Treatment for sleep apnea depends on the type diagnosed, its severity, and how well a patient responds to specific approaches.
Most people find that a combination of methods works better than relying on a single solution.
1. CPAP Therapy
CPAP therapy delivers a steady stream of pressurized air through a mask worn during sleep, keeping the airway open and preventing breathing interruptions.
It is the most widely prescribed treatment for obstructive sleep apnea and works effectively across mild, moderate, and severe cases.
It does not cure the condition but eliminates most apnea events when used consistently every night.
2. BiPAP Therapy
BiPAP therapy uses two separate pressure levels, one for inhaling and a lower one for exhaling, making it easier to breathe against the airflow.
It is commonly prescribed for central sleep apnea, complex sleep apnea, or patients who find standard CPAP pressure difficult to tolerate.
The dual pressure design also makes it a preferred option for people with underlying lung conditions.
3. Adaptive Servo-Ventilation (ASV)
ASV is an advanced PAP device that monitors your breathing patterns in real time and automatically adjusts pressure to prevent pauses before they happen.
It is designed specifically for complex and central sleep apnea, in which breathing irregularities are unpredictable and standard pressure settings fall short.
Most sleep specialists consider it the most precise non-surgical option for difficult-to-treat cases.
4. Oral Appliance Therapy
A custom-fitted oral appliance, known as a mandibular advancement device, repositions the jaw and tongue slightly forward to prevent the airway from collapsing during sleep.
It is a practical alternative for patients with mild to moderate obstructive sleep apnea who cannot tolerate PAP therapy.
A dentist trained in sleep medicine fits and adjusts the device across several follow-up appointments.
5. Inspire Therapy (Hypoglossal Nerve Stimulation)
Inspire is an FDA-approved implantable device that stimulates the hypoglossal nerve to keep the tongue and airway open throughout the night.
The patient activates it with a small handheld remote before going to sleep.
It is intended for patients with moderate to severe obstructive sleep apnea who have not responded adequately to CPAP and has shown strong results in long-term clinical studies.
6. Positional Therapy
Positional therapy targets people whose sleep apnea occurs mainly or entirely when sleeping on their back, a pattern known as positional obstructive sleep apnea.
Wearable devices, vibration-based trainers, and specially shaped pillows prompt the sleeper to shift position without fully waking.
It is most effective as a complementary treatment alongside CPAP or oral appliance therapy rather than a complete standalone solution.
7. Surgical Options
Surgery is considered when structural issues in the airway are directly causing obstruction or when other treatments have not produced adequate results.
Uvulopalatopharyngoplasty removes excess throat tissue to widen the airway, while maxillomandibular advancement permanently repositions the jaw for a larger opening.
Outcomes depend heavily on the specific procedure chosen and the individual anatomy of the patient.
8. Lifestyle Modifications
Weight loss, reduced alcohol consumption, quitting smoking, and maintaining a consistent sleep schedule can meaningfully lower sleep apnea severity, especially in mild to moderate obstructive cases.
These changes rarely resolve the condition entirely on their own but can reduce the pressure settings needed on PAP devices and improve overall treatment response.
They are typically recommended alongside medical treatment rather than as a replacement.
Treatment Based on Type
Because each type of sleep apnea has a different root cause, treatment is never one-size-fits-all. Here is a quick breakdown of how each type is typically managed:
| Type | Primary Treatment | Additional Notes |
|---|---|---|
| Obstructive Sleep Apnea (OSA) | CPAP therapy | Delivers continuous pressurized air to keep the airway open throughout the night |
| Central Sleep Apnea (CSA) | Treat the underlying cause | May include managing heart failure, adjusting medications, or supplemental oxygen |
| Complex Sleep Apnea | Adaptive servo-ventilation (ASV) | Adjusts airflow in real time to respond to both obstructive and central events |
| Sleep-Related Hypoventilation | Bilevel positive airway pressure (BiPAP) | Weight management and treating lung or neuromuscular conditions also play a key role |
Getting the right diagnosis is what makes the right treatment possible.
A sleep specialist can review your results and recommend the most appropriate path based on your specific type and severity.
Risk Factors for Sleep Apnea
Several physical, lifestyle, and genetic factors can raise your likelihood of developing sleep apnea.
- Excess Weight: Fat deposits around the neck narrow the airway and make collapse during sleep more likely.
- Neck Circumference: A neck circumference above 17 inches in men and 16 inches in women is a recognized clinical risk indicator.
- Age: Throat muscle tone decreases naturally with age, making airway collapse more common in adults over 40.
- Sex: Men are two to three times more likely to develop sleep apnea, though the gap narrows after menopause in women.
- Family History: Genetic predisposition related to airway anatomy can increase risk even without obvious symptoms.
- Nasal Congestion and Airway Anatomy: A deviated septum, enlarged tonsils, or a narrow airway can reduce the available airflow space during sleep.
- Alcohol and Sedative Use: Both relax throat muscles beyond normal levels, increasing apnea frequency and duration overnight.
- Smoking: Causes airway inflammation and fluid retention that narrows the passage and disrupts breathing during sleep.
Knowing your risk factors helps you and your doctor act earlier and with more precision.
When to See a Doctor
Sleep apnea does not resolve on its own, and the longer it goes unaddressed, the more it affects your health and quality of life.
If you or someone close to you has noticed persistent snoring, breathing pauses during sleep, or extreme daytime tiredness that does not improve with rest, those are signs worth taking seriously.
Untreated sleep apnea puts long-term strain on the heart, raises blood pressure, and affects focus and mood over time.
It is very manageable once properly diagnosed. A conversation with your doctor and a sleep study can give you the clarity and direction you need to start sleeping and feeling better.
Frequently Asked Questions
What are the 4 Types of Sleep Apnea?
The four types are obstructive, central, complex, and sleep-related hypoventilation.
Which Type Is Most Common?
Obstructive sleep apnea is the most common form, caused by airway blockage during sleep.
How is Sleep Apnea Diagnosed?
Sleep apnea is diagnosed through a sleep study that measures breathing interruptions and oxygen levels.





